





Good Friday is a tough day for a Christian. It is a day of weeping and mourning; of venerating the Cross and meditating on the terrible reality of Christ’s tortuous death. It is an annual memorial service for a loved one, and the pain and grief is never made any easier because the reality of the Cross is fresh and relevant and immediate in the life of the believer: it is a moment that transcends time and space and is as real this year as it was in the thirty-third and final year of Christ’s life. It is also traditionally a day of intentional and serious fasting - mainly a diet of water and weeping for me. So, by the evening you’re wiped out and just want a bit of rest, perhaps relaxing in front of a film; that is certainly how I feel. Yet every Christian wants to spend the day focused on the Passion of Jesus, so not just any old film will do - it ought to be a film that allows us to keep Jesus’s sacrifice in mind. Below are my top five tips for a Good Friday evening watch… popcorn to be eaten plain, or salted with tears if you must!
5 - The Passion of the Christ
The obvious choice. Controversial upon release for its depiction of the Temple hierarchy and the bloody violence with which it depicts Christ’s scourging and Crucifixion, it lives now in a certain ignominy. I would argue it deserves a reappraisal. Gibson is a solid director, takes the work seriously, and gives us a good-looking film. Jim Caviezel gives a terrific central performance (that makes you think he deserved a better career for the last twenty years), and all the cast put in good turns. However, it's the interpretation of the meaning of the death of Christ that intrigues me. When it first hit the screens, some saw it as a bloody expression of the view that Jesus dies to appease God’s wrath. Yet Gibson carefully intersperses scenes of the Last Supper with the scenes of torture, makes Satan a demonic inversion of the Madonna and Child, and constantly makes clear that it is the power of love and not anger or cruelty that is conquering the world. It is brutal and horrific (and so in fifth place) - but so is capital punishment… so maybe we need to endure it. In this film you can find many nuances of the Christian idea of love and redemption and salvation etched upon the screen.
4 - The Shawshank Redemption

A less obvious choice, and a film in which there is no vicarious death, but bear with me. Frank Darabont's epic drama sees Andy Dufresne (Tim Robbins) locked up for a crime he did not commit. Over the decades he learns how to navigate the dangers of prison life, makes friends and enemies, and becomes implicated in a great web of corruption. His great supporter and confidant is ‘Red’ (Morgan Freeman), who is the only man in Shawshank Prison who will admit his murderous guilt. This is one of those films that it's hard not to love, and you’ve probably seen it so many times before that it is the cinematic equivalent of a comforting takeaway. Under the surface of some terrific performances, masterful direction, and a heart-tugging score, the film is full of Christian themes. The innocent man punished for the sins of another, the death of Andy’s ego as he learns to find purpose in improving the lives of his fellow inmates, the dark powers of corruption brought to justice, and a man descending in the very bowels (the right word if you know the escape scene) of hell and emerging clean and reborn. Its aged beautifully, and inaugurated the Freeman voiceover as a staple of cinematic culture.
3 - The Gospel According to St Matthew
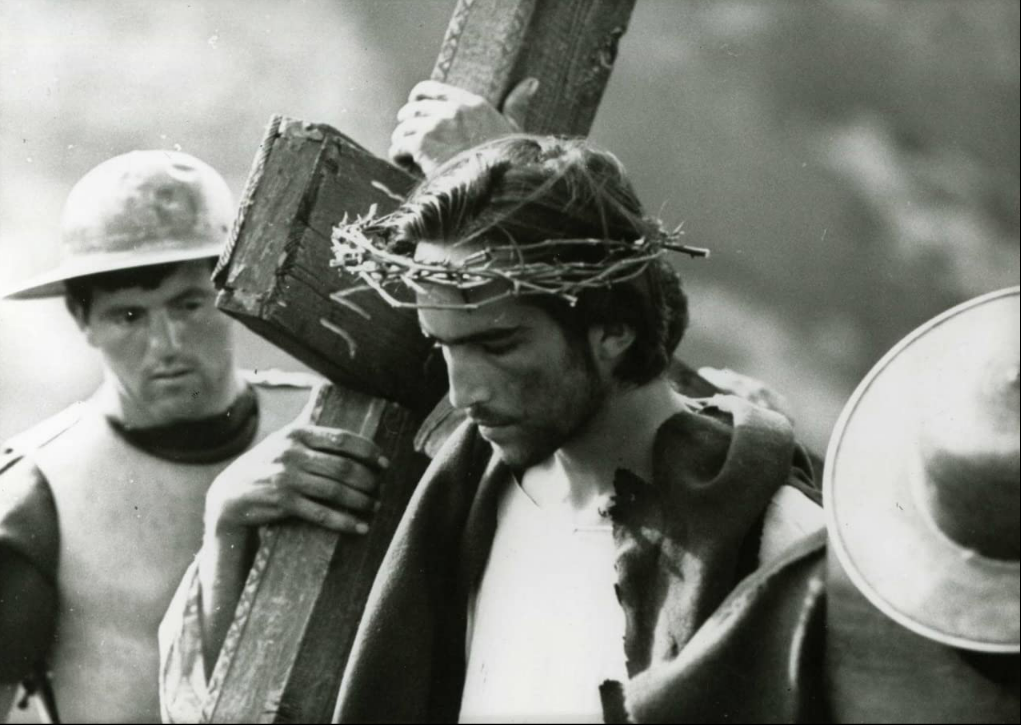
Approved by the Vatican and made by a director in his prime wrestling with his faith, Pasolini’s masterpiece is a sumptuous black-and-white exploration of the life of Christ. The entire film is saturated with the sense of living in the poverty of first-century Palestine. Static close ups jump-cutting between one another disorient the viewer and give the impression that the supernatural is taking over the world we are seeing. It is hardly dynamic by the standards of a modern Passion film, but this is to its great benefit. Pasolini lends the film an Italian neo-realist flair that makes it seem almost like one is watching a documentary. The great joy of The Gospel is that it is a telling of the full Gospel, rather than the Passion in isolation. We see Jesus grow into manhood and into ministry, we see the shocking impact of his radical teaching, we see the conspiracy, and so when the Crucifixion of Jesus does happen it is remarkably impactful while also seeming ‘right’. We see how such a Gospel of radical devotion to God and love of neighbour does terrify a world that thinks in terms of power, and we see the great victory that the Cross really is.
2 - Gran Torino

Clint Eastwood playing a role of a lifetime, and teaching us what loving one’s neighbour really looks like… what more could you want. Eastwood plays Walt: a widower, and veteran, a retired blue-collar worker, and an inveterate racist and tobacco user. Walt is embittered and alone, disgusted by the state of his Detroit neighbourhood, which has morphed from an all-white working-class community to a mainly Asian community blighted by gang violence. One night Walt saves his young neighbour from a forced gang initiation, and grudgingly becomes a mentor and quasi-father-figure to the boy, and soon his sister. Walt has no desire to connect with the world outside, but does so out of a sense of discipline and duty, and this is an excellent corrective to modern sentimental notions of love. On the Cross, Christ performs the most perfect act of love, offering forgiveness even to his executioners… it is unlikely that in that moment Jesus liked them. In the Gospel narratives Jesus is often frustrated to the point of anger, with the stubbornness of his hearers, and the lack of understanding of his disciples. Jesus doesn’t always like them, but he does love them. In the climactic scene of the film Walt resolves to make a great sacrifice to protect his community - a community he doesn’t really like anymore. This is real love, the love of the Cross. It does not emanate from fleeting and flighty emotionalism, but from a tremendous act of dedication and will. Eastwood gives us a great Good Friday lesson in love, and his performance is superb.
1 - The Last Temptation of the Christ
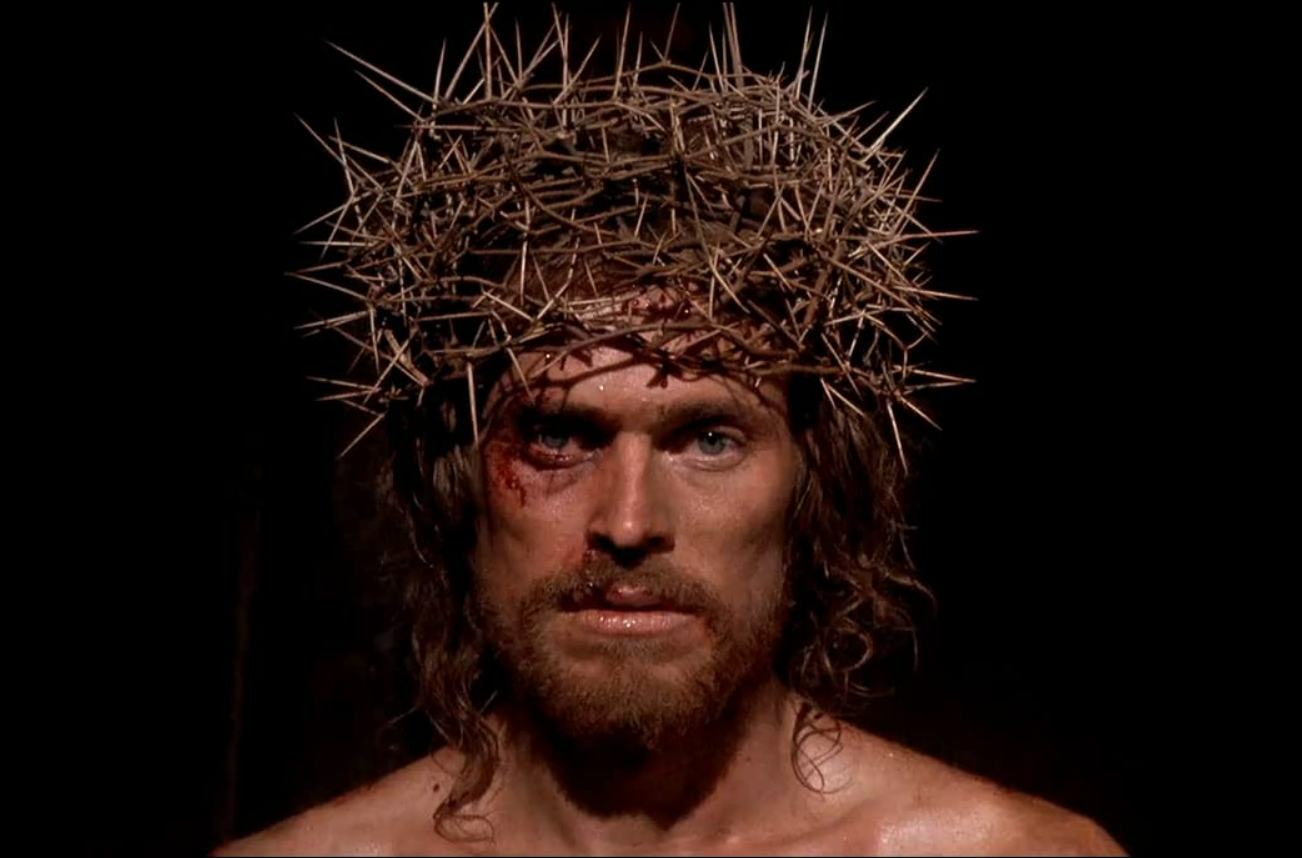
My number one pick is a mammoth of visual spectacle and a roller-coaster of emotions. Martin Scorsese has always been fascinated with the Catholic faith that he can’t quite embrace, and many of his most interesting and personal films have had the Christian narrative of redemption woven through. In 'Temptation' he tackles the subject head on, and gives us a religious epic to rival any Charlton Heston flick. Willem Defoe is a lean, wild eyed, and manic Jesus - plagued by doubt and anxiety and horrific migraines that could be demonic…or they could be God. Scorsese and Defoe work together to present the ministry of Jesus in very human terms. Christ is a psychologically complex man who is struggling to cope with his mission in a world that is so very broken. Much like Pasolini’s Gospel, this is a film that takes the supernatural seriously. Nothing is ever just what it is. There is no weather event or vision or animal encounter that is not suffused with eternal meaning. The film touches on every emotion: from furious anger, to heart-rending sadness, to uproarious laughter (to this day I can’t see a priest friend of mine without shouting ‘Judith’ and bursting into laughter). The closing acts of the film allow us to see just what Christ was sacrificing on the Cross - not just the life he had led, but the life he could have led. Christ is tempted to the very end, with the worst psychological torment possible, and still he remains faithful to the end. Scorsese may not know exactly where he stands before God, but he was graced with the talent to give the world a remarkably evocative take on the Passion of Jesus.
